Title
題目
SpinFlowSim: A blood flow simulation framework for histology-informeddiffusion MRI microvasculature mapping in cancer
SpinFlowSim:用于癌癥組織學信息驅動的擴散MRI微血管映射的血流模擬框架
01
文獻速遞介紹
在擴散磁共振成像(dMRI)中,水質子的運動通過磁場梯度編碼到采集的信號中(Kiselev, 2017)。擴散編碼不僅對純擴散引起的布朗運動敏感,還對血流質子通過復雜毛細血管網絡的非相干流動所產生的偽擴散效應敏感(Le Bihan 等, 1986)。通過偽隨機分布毛細血管的流動會導致dMRI信號幅度衰減,這一現象被稱為體素內不相干運動(IVIM)效應。IVIM使得通過dMRI在體表征微血管灌注成為可能(Le Bihan, 2019),這在多種疾病中具有重要意義,例如癌癥(Fokkinga 等, 2024)。癌癥的特征是異常的微血管系統,其血流模式可能與正常組織有顯著差異(Munn, 2003)。腫瘤血管是抗血管生成治療的特定靶點,這類治療已應用于多種癌癥(如肝癌或腎癌(Jayson 等, 2016)),并正在與免疫檢查點抑制劑等療法聯合測試,取得了有希望的結果(Huinen 等, 2021)。通過dMRI對血管特性進行非侵入性評估,可為醫生提供腫瘤表征和縱向評估的新工具。因此,這是一個活躍的研究領域,研究范圍從惡性腫瘤檢測到治療反應評估(Iima 等, 2018; Perucho 等, 2021)。 IVIM方法通常依賴于從血管外組織dMRI信號中分離出血管信號(Barbieri 等, 2016b,a)。多指數模型常用于此目的,提供諸如血管信號分數f_v或偽擴散(血管)表觀擴散系數(ADC)D?等指標,最近通過深度學習已使這些指標的估計更加穩健(Barbieri 等, 2020; Zheng 等, 2023)。f_v和D?都是有用的指標,因為它們在癌癥評估中已顯示出價值(Dappa 等, 2017)。然而,這些指標存在局限性,因為它們將多種不同的微血管特征糾纏為單個數值,例如在擴散流動狀態下血流速度平均值與毛細血管長度分布的乘積(Le Bihan 和 Turner, 1992-09)。此外,它們不考慮擴散衰減的高階累積量(例如與b2成比例的峰度項),且其實際數值可能以復雜的方式依賴于采集協議(Wu 和 Zhang, 2019)。實際上,這使得常規IVIM指標成為半定量的替代參數,這一事實連同其已知的高可變性(Barbieri 等, 2020),阻礙了它們的大規模臨床應用。 最近,在組織學真實的體素模型中對dMRI信號進行數值模擬正越來越多地用于指導參數估計(Nilsson 等, 2010; Nguyen 等, 2014; Fieremans 和 Lee, 2018; Buizza 等, 2021; Morelli 等, 2023)。模擬指導的方法增加了信號模型的真實性,從而可能提高dMRI參數圖的生物學保真度(Nedjati-Gilani 等, 2017; Palombo 等, 2019)。然而,迄今為止,dMRI模擬主要由蒙特卡洛布朗隨機游走主導(Hall 和 Alexander, 2009; Ginsburger 等, 2019; Rafael-Patino 等, 2020; Lee 等, 2021)。鑒于只有少數模擬框架專注于血流(Van 等, 2021; Weine 等, 2024),迫切需要針對血流產生的dMRI信號、具有組織學意義且可重復的新型模擬器。這些模擬器可用于指導基于dMRI的非侵入性微血管映射新數值方法,為臨床環境中的腫瘤學家提供具有生物學意義的血管標志物。新的dMRI方法可實現對經典IVIM f_v和D?未捕捉到的毛細血管流動模式的表征,例如提供關于各向異性流動模式、高階累積量或血管信號擴散時間依賴性的信息。 本文旨在填補這一科學空白。我們提出了一個用于血管網絡內血流模擬的開源框架,此后稱為SpinFlowSim,并展示了其在dMRI中指導微血管特性估計的潛力。我們首先闡述SpinFlowSim背后基于管道網絡理論的計算引擎,然后描述從人類腫瘤組織學圖像獲得的真實血管網絡內流動產生的dMRI信號的合成過程。最后,我們通過使用合成信號指導微血管特性估計,展示了SpinFlowSim的潛在應用,該應用在健康志愿者和癌癥患者中通過計算機模擬和體內實驗進行了驗證。初步研究結果已以摘要形式在會議上發表(Voronova 等, 2024b),本文的草稿也已作為預印本發布在medRxiv服務器上(Voronova 等, 2024a)。
Abatract
摘要
Diffusion Magnetic Resonance Imaging (dMRI) sensitises the MRI signal to spin motion. This includes Browniandiffusion, but also flow across intricate networks of capillaries. This effect, the intra-voxel incoherent motion(IVIM), enables microvasculature characterisation with dMRI, through metrics such as the vascular signalfraction 𝑓𝑉 or the vascular Apparent Diffusion Coefficient (ADC) 𝐷? . The IVIM metrics, while sensitive toperfusion, are protocol-dependent, and their interpretation can change depending on the flow regime spinsexperience during the dMRI measurements (e.g., diffusive vs ballistic), which is in general not known for agiven voxel. These facts hamper their practical clinical utility, and innovative vascular dMRI models are neededto enable the in vivo calculation of biologically meaningful markers of capillary flow. These could have relevantapplications in cancer, as in the assessment of the response to anti-angiogenic therapies targeting tumourvessels. This paper tackles this need by introducing SpinFlowSim, an open-source simulator of dMRI signalsarising from blood flow within pipe networks. SpinFlowSim, tailored for the laminar flow patterns withincapillaries, enables the synthesis of highly-realistic microvascular dMRI signals, given networks reconstructedfrom histology. We showcase the simulator by generating synthetic signals for 15 networks, reconstructedfrom liver biopsies, and containing cancerous and non-cancerous tissue. Signals exhibit complex, non-monoexponential behaviours, consistent with in vivo signal patterns, and pointing towards the co-existence ofdifferent flow regimes within the same network, as well as diffusion time dependence. We also demonstratethe potential utility of SpinFlowSim by devising a strategy for microvascular property mapping informed bythe synthetic signals, and focussing on the quantification of blood velocity distribution moments and of anapparent network branching* index. These were estimated in silico and in vivo, in healthy volunteers scanned at1.5T and 3T and in 13 cancer patients, scanned at 1.5T. In conclusion, realistic flow simulations, as thoseenabled by SpinFlowSim, may play a key role in the development of the next-generation of dMRI methods formicrovascular mapping, with immediate applications in oncology.
擴散磁共振成像(dMRI)可使MRI信號對自旋運動敏感,這其中既包括布朗擴散,也涵蓋了通過復雜毛細血管網絡的血流運動。這種效應即體素內不相干運動(IVIM),它使得利用dMRI表征微血管成為可能,具體可通過血管信號分數𝑓𝑉或血管表觀擴散系數(ADC)𝐷?等指標實現。盡管IVIM指標對灌注敏感,但其結果依賴于成像協議,并且其解讀會因dMRI測量過程中自旋所處的血流狀態(如擴散型 vs 彈道型)而變化——而對于給定體素,這種狀態通常是未知的。這些因素阻礙了其在臨床實踐中的應用,因此需要創新的血管dMRI模型來實現體內毛細血管血流生物學標志物的計算。這類模型可能在癌癥領域具有重要應用,例如評估針對腫瘤血管的抗血管生成療法的響應情況。 本文針對這一需求,引入了SpinFlowSim——一種針對管道網絡內血流的開源dMRI信號模擬器。SpinFlowSim專為毛細血管內的層流模式設計,在給定從組織學重建的網絡結構時,能夠合成高度逼真的微血管dMRI信號。我們通過為15個從肝活檢中重建的、包含癌組織和非癌組織的網絡生成合成信號來展示該模擬器的能力。這些信號表現出復雜的非單指數行為,與體內信號模式一致,表明同一網絡內存在不同血流狀態,且與擴散時間相關。 此外,我們還通過設計一種基于合成信號的微血管特性映射策略,重點量化血流速度分布矩和表觀網絡分支指數,展示了SpinFlowSim的潛在應用價值。這些指標在健康志愿者(1.5T和3T掃描)和13例癌癥患者(1.5T掃描)中通過計算機模擬和體內實驗進行了估計。 綜上所述,SpinFlowSim所實現的真實血流模擬可能在下一代dMRI微血管映射方法的開發中發揮關鍵作用,并可立即應用于腫瘤學領域。
Method
方法
In this section we illustrate the computational engine upon whichSpinFlowSim relies, illustrated in Fig. 1. Afterwards, we present thehistological data used to generate realistic vascular networks, and thendescribe how synthetic dMRI signals were used to inform microvasculature parameter estimation in silico and in vivo.
在本節中,我們將闡釋SpinFlowSim所依賴的計算引擎(如圖1所示)。隨后,我們將介紹用于生成真實血管網絡的組織學數據,并描述如何利用合成的dMRI信號在計算機模擬和體內實驗中指導微血管參數估計。
Conclusion
結論
SpinFlowSim, our open-source, freely-available python simulator ofblood micro-perfusion in capillaries, enables the synthesis and characterisation of realistic microvascular dMRI signals. Perfusion simulationsin vascular networks reconstructed from histology may inform the noninvasive, numerical estimation of innovative microvascular propertiesthrough dMRI, whose feasibility is demonstrated herein in vivo inhealthy subjects and in cancer patients.
SpinFlowSim是我們開發的開源Python模擬器,可免費獲取,用于模擬毛細血管中的血液微灌注,能夠合成和表征真實的微血管dMRI信號。從組織學重建的血管網絡中進行灌注模擬,可通過dMRI為無創、數字化估計新型微血管特性提供依據,其可行性已在健康受試者和癌癥患者的體內實驗中得到驗證。
Results
結果
3.1. Vascular networks
Fig. 2 illustrates the 15 vascular networks generated in this studyfrom liver tumour biopsies. Out of the total, 3 were segmented onnon-cancerous liver parenchyma, while the remaining 12 on canceroustissue. The 3 non-cancerous networks were drawn on liver tissue foundon the histological slide, adjacent to tumour tissue (n = 2 melanomametastases; n = 1 ovarian cancer metastasis). The 12 networks drawnon cancerous tissue came from primary liver hepatocellular carcinoma(HCC, n = 5), or from liver metastases of colorectal cancer (CRC, n = 5),endometrial cancer (n = 1), and melanoma (n = 1).Table 1 reports salient statistics of the vascular networks shown inFig. 2, related to capillary radii, length, velocity distribution, number ofvascular segments sensed by flowing spins and number of input/outputpaths. None of the networks contain close loops, and all capillarysegments are always part of at least one flow path connecting the inletto the outlet. The network size varies from approximately 240 to up to600 μm. The number of segments varies from 42 to 77, while the meaninput/output path length from approximately 316 to 753 μm. The tableshows that different network morphologies lead to different blood velocity distributions. For example, mean 𝑣𝑚 across VFR realisations canvary from as low as approximately 4 mm/s up to 25 mm/s. This rangeof variation is mirrored in the average number of capillaries bloodtravels through during the simulation (𝐴𝑁𝐵 metric), which varies fromjust over 12 up to almost 57 segments (note that in some cases, 𝐴𝑁𝐵can be slightly higher than the total number of segments, given thatspins reaching the outlet of the network continue flowing in a copy ofthe network itself). The mean path length 𝑃 𝐿𝑚 also varies considerably,e.g., from just over 300 μm for network 3, exhibiting the fastest flowamong networks, to up to roughly 700 μm, as in networks 5 or 6.
圖2展示了本研究從肝腫瘤活檢中生成的15個血管網絡。其中3個分割自非癌性肝實質,其余12個來自癌組織。3個非癌性網絡取自組織學切片上鄰近腫瘤組織的肝組織(2例黑色素瘤轉移灶,1例卵巢癌轉移灶)。12個癌組織來源的網絡中,5例為原發性肝細胞癌(HCC),5例為結直腸癌(CRC)肝轉移灶,1例子宮內膜癌和1例黑色素瘤肝轉移灶。 ? 表1報告了圖2中血管網絡的關鍵統計數據,包括毛細血管半徑、長度、速度分布、血流自旋感知的血管節段數量及輸入/輸出路徑數量。所有網絡均無閉合環路,且所有毛細血管節段至少屬于一條連接入口與出口的血流路徑。網絡尺寸約為240-600 μm,節段數量為42-77個,平均輸入/輸出路徑長度約316-753 μm。 ? 表中顯示,不同網絡形態導致血流速度分布差異顯著。例如,不同體積流量率(VFR)下的平均血流速度𝑣**𝑚范圍為4-25 mm/s,這一變化范圍與模擬中血液流經的平均毛細血管數量(𝐴𝑁𝐵指標)一致,其值為12-57個節段(需注意,由于自旋到達網絡出口后會繼續在復制網絡中流動,部分情況下𝐴𝑁𝐵可能略高于總節段數)。平均路徑長度𝑃𝐿**𝑚也存在較大差異,如流速最快的網絡3約為300 μm,而網絡5和6可達700 μm。
Figure
圖
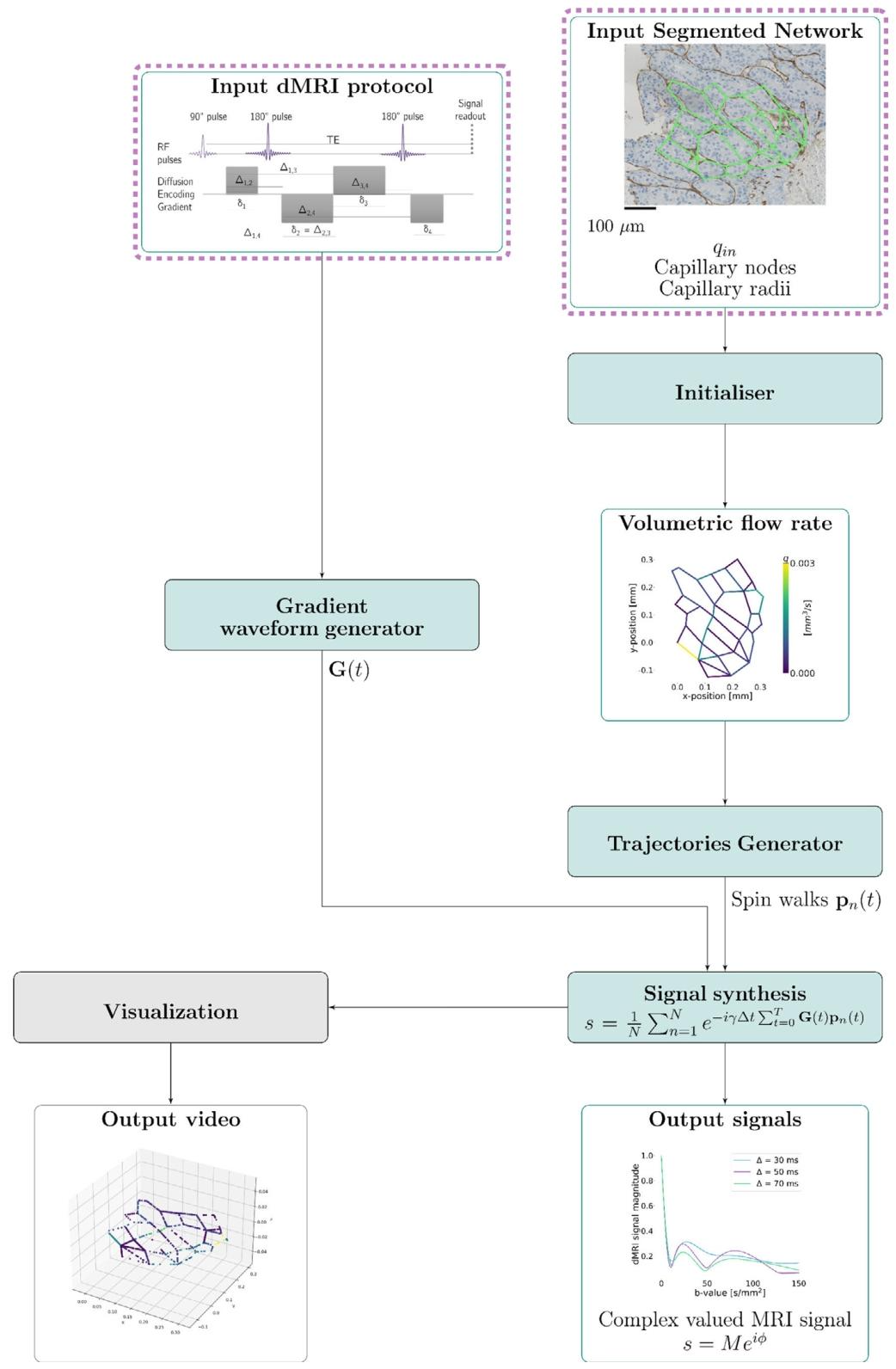
Fig. 1. Outline of the proposed SpinFlowSim framework. The dashed boxes indicate user-provided input information. An illustrative example of a network segmented on a biopsywith resolved volumetric flow rates for an input flow 𝑞𝑖𝑛 = 3.1 ? 10?3 mm3/s and synthesised signals are shown.
圖1. 所提出的SpinFlowSim框架概述。虛線框表示用戶提供的輸入信息。圖中展示了一個在活檢樣本上分割的網絡示例,其輸入流量𝑞𝑖𝑛 = 3.1?10?3 mm3/s時的解析體積流量率,以及合成的信號。

Fig. 2. Vascular networks segmented on digitised liver tumour biopsies (resolution: 0.454 μm). Each network is labelled as ‘‘Non-Cancerous’’ or ‘‘Cancerous’’, depending on whetherit was drawn on non-cancerous liver parenchyma or on tumour tissue. For the latter case, the primary cancer is also indicated (CRC stands for Colorectal Cancer, while HCCfor Hepatocellular Carcinoma). The non-cancerous networks were drawn on liver tissue found on liver tumour biopsies of patients suffering from Melanoma (n = 2) and Ovariancancer (n = 1)
圖2. 從數字化肝腫瘤活檢樣本中分割的血管網絡(分辨率:0.454 μm)。每個網絡根據其繪制于非癌性肝實質還是腫瘤組織,標記為“非癌性”或“癌性”。對于癌性情況,還會注明原發癌類型(CRC代表結直腸癌,HCC代表肝細胞癌)。非癌性網絡取自黑色素瘤患者(n=2)和卵巢癌患者(n=1)肝腫瘤活檢樣本中的肝組織。
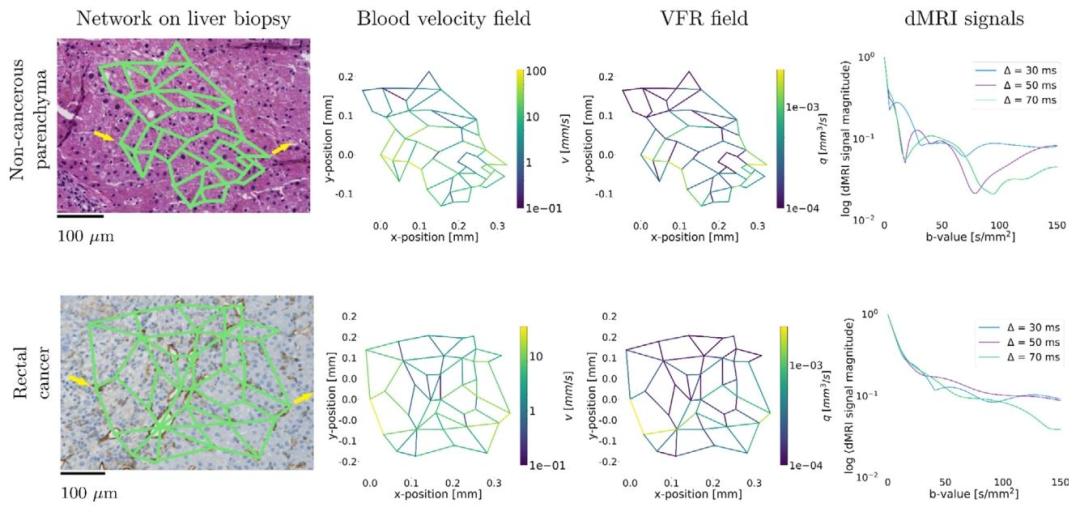
Fig. 3. Examples of resolved vascular networks. The top row shows results from a vascular network segmented on a HE-stained non-cancerous liver region, found on a biopsy ofa patient with metastatic melanoma (Net 6). The bottom panel shows results from a CD31-stained rectal cancer area (Net 12). From left to right, we show the vascular network,the resolved blood flow velocity field for 𝑞𝑖𝑛 = 3.1 ? 10?3 mm3/s, and examples of dMRI signal decay over a range of b-values (0–150 s∕mm2 ) and diffusion times (𝛥 = {30, 50,70} ms, 𝛿 = 20 ms). The inlet/outlet were: nodes 0 and 33 for Net 6; nodes 0 and 14 for Net 12. These have been indicated by input/output yellow arrows.
圖3. 解析血管網絡示例。頂行顯示了從轉移性黑色素瘤患者活檢樣本中HE染色的非癌性肝區域分割的血管網絡結果(網絡6)。底行顯示了CD31染色的直腸癌區域結果(網絡12)。從左到右依次為:血管網絡、輸入流量𝑞**𝑖𝑛 = 3.1?10?3 mm3/s時的解析血流速度場,以及在b值范圍(0–150 s/mm2)和擴散時間(𝛥 = {30, 50, 70} ms,𝛿 = 20 ms)下的dMRI信號衰減示例。網絡6的入口/出口為節點0和33;網絡12為節點0和14,已通過輸入/輸出黃色箭頭標注。

Fig. 4. Scatter plots relating estimated and ground truth microvascular parameters in computer simulations. First row (panels (a), (b), (c)): results for protocol ‘‘PGSE in vivo’’.Second row (panels (d), (e), (f)): results for protocol ‘‘TRSE’’. Third row (panels (g), (h), (i)): results for protocol ‘‘richPGSE subset’’. Fourth row (panels (j), (k), (l)): results forprotocol ‘‘richPGSE’’. From left to right: results for metric 𝑣𝑚 (panels (a), (d), (g), (j)); results for metric 𝑣𝑠 (panels (b), (e), (h), (k)); results for metric 𝐴𝑁𝐵 (panels (c), (f), (i),(l)).Spearman’s and Pearson’s correlation coefficients between estimated and ground truth values are also reported in each plot
圖4. 計算機模擬中估計微血管參數與真實值的散點圖。第一行(圖(a)、(b)、(c)):“體內PGSE”協議結果;第二行(圖(d)、(e)、(f)):“TRSE”協議結果;第三行(圖(g)、(h)、(i)):“richPGSE子集”協議結果;第四行(圖(j)、(k)、(l)):“richPGSE”協議結果。從左至右分別為:𝑣𝑚指標(圖(a)、(d)、(g)、(j))、𝑣**𝑠指標(圖(b)、(e)、(h)、(k))、𝐴𝑁𝐵指標(圖(c)、(f)、(i)、(l))。各圖中還報告了估計值與真實值的斯皮爾曼和皮爾遜相關系數。

Fig. 5. Representative vascular voxel signals measured in two healthy volunteers in vivo. Top (A–D): signals from healthy volunteer 4, scanned on a 3T system, with the ‘‘PGSEinvivo’’protocol, based on routine PGSE. Bottom (E–H): signals from healthy volunteer 2, scanned on a 1.5T system, with the ‘‘TRSEinvivo’’ protocol, based on a DW TRSE acquisition.From left to right, signals from different ROIs are shown: kidney cortex (A and E); kidney medulla (B and F); spleen (C and G); liver parenchyma (D and H). The figure reportsthe median and the inter-quartile range of variation of the signal across voxels within the ROI. An estimated range of noise floor fluctuations is also reported in grey
圖5. 兩名健康志愿者體內測得的代表性血管體素信號。頂部(A-D):健康志愿者4在3T系統上采用基于常規PGSE的“體內PGSE”協議掃描的信號。底部(E-H):健康志愿者2在1.5T系統上采用基于DW TRSE采集的“體內TRSE”協議掃描的信號。從左到右顯示不同ROI的信號:腎皮質(A和E);腎髓質(B和F);脾臟(C和G);肝實質(D和H)。圖中報告了ROI內體素信號的中位數和四分位距變化范圍,灰色區域還報告了噪聲本底波動的估計范圍。

Fig. 6. Microvascular maps in a representative healthy volunteer scanned on the 1.5T system with protocol ‘‘TRSEinvivo’’. (a): labelled scan; (b) and (c): IVIM maps 𝑓**𝑉 and 𝐷 ;(d), (e) and (f): microvascular indices 𝑣𝑚 , 𝑣𝑠 and 𝐴𝑁𝐵. In the labelled scan, we highlight the location of the liver and the spleen
圖6. 一名代表性健康志愿者在1.5T系統上采用“體內TRSE”協議掃描的微血管圖。(a):標記掃描圖;(b)和(c):IVIM參數圖𝑓𝑉和𝐷?;(d)、(e)和(f):微血管指數𝑣𝑚、𝑣𝑠和𝐴𝑁𝐵。在標記掃描圖中,我們標出了肝臟和脾臟的位置。

Fig. 7. Microvascular maps in the healthy volunteer scanned on the 3T system with protocol ‘‘PGSEinvivo’’. (a): labelled scan; (b) and (c): IVIM maps 𝑓𝑉 and 𝐷? ; (d), (e) and(f): microvascular indices 𝑣𝑚 , 𝑣𝑠 and 𝐴𝑁𝐵. In the labelled scan, we highlight the location of the liver, the spleen and of the kidneys.
圖7. 健康志愿者在3T系統上采用“體內PGSE”協議掃描的微血管圖。(a):標記掃描圖;(b)和(c):IVIM參數圖𝑓𝑉和𝐷?;(d)、(e)和(f):微血管指數𝑣𝑚、𝑣𝑠和𝐴𝑁𝐵。在標記掃描圖中,我們標出了肝臟、脾臟和腎臟的位置。

Fig. 8. Bar plots reporting mean and standard error of the mean of all microvascular metrics in the different regions-of-interest (ROIs) of the four healthy volunteers. (a): trendsfor metric 𝑓𝑉 ; (b): trends for metric 𝐷? ; (c): trends for metric 𝑣𝑚 ; (d): trends for metric 𝑣𝑠 ; (e): trends for metric 𝐴𝑁𝐵.
圖8. 柱狀圖展示了四名健康志愿者不同感興趣區域(ROI)中所有微血管指標的均值和均值標準誤差。(a):血管信號分數𝑓𝑉的趨勢;(b):血管表觀擴散系數𝐷?的趨勢;(c):血流速度均值𝑣𝑚的趨勢;(d):血流速度標準差𝑣𝑠的趨勢;(e):表觀網絡分支指數𝐴𝑁𝐵的趨勢。
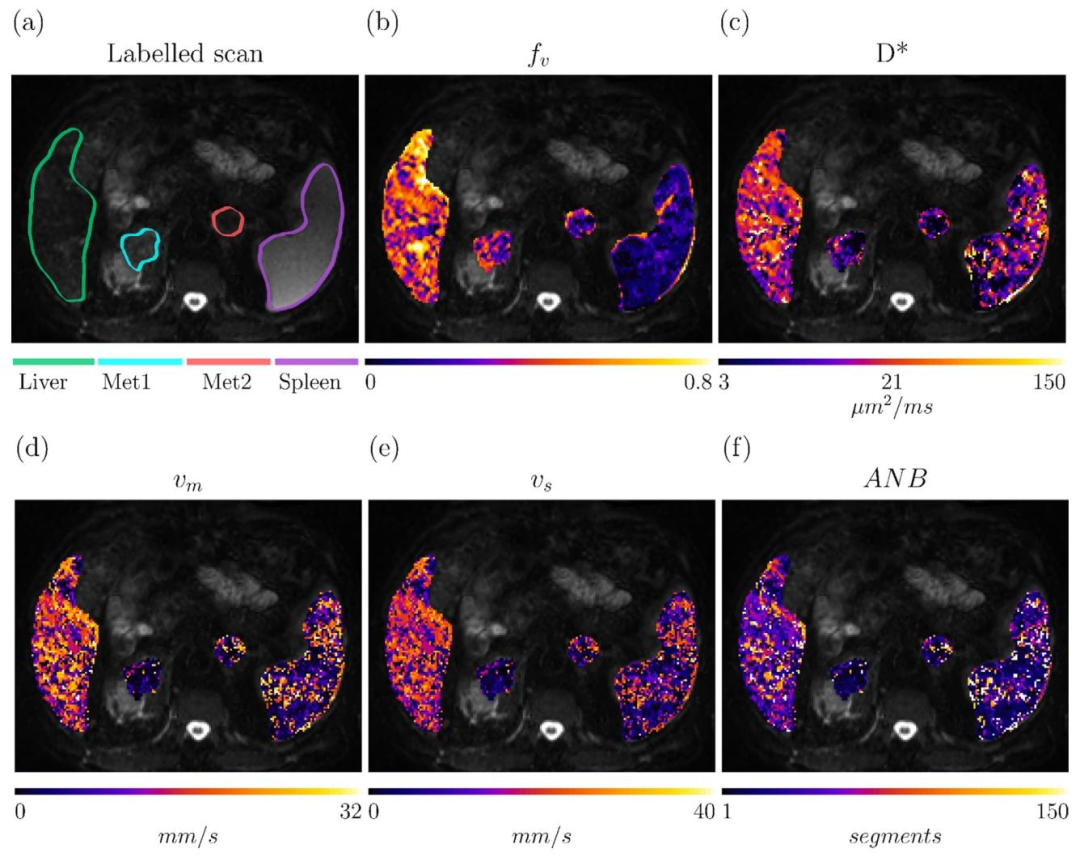
Fig. 9. Parametric maps obtained in adrenal metastases, liver and spleen of a 61 y.o. male patient, suffering from advanced rectal cancer (patient 8, scanned on a 1.5T SiemensAvanto system with a DW TRSE sequence). Top row: labelled scan and IVIM maps 𝑓𝑉 and 𝐷? . Bottom row: microvascular parameters obtained via simulation-informed modelfitting, namely: mean blood velocity 𝑣𝑚 , blood velocity standard deviation 𝑣𝑠 , and Apparent Network Branching 𝐴𝑁𝐵.
圖9. 一名61歲晚期直腸癌男性患者(患者8,使用1.5T西門子Avanto系統通過DW TRSE序列掃描)腎上腺轉移灶、肝臟和脾臟的參數圖。頂行:標記掃描圖及IVIM參數圖𝑓𝑉(血管信號分數)和𝐷?(血管表觀擴散系數)。底行:通過模擬指導模型擬合獲得的微血管參數,即血流速度均值𝑣𝑚、血流速度標準差𝑣𝑠和表觀網絡分支指數𝐴𝑁𝐵。
Table
表

Table 1Summary of vascular networks with corresponding microvascular properties generated for this study. The non-cancerous networks were drawn on non-cancerous liver tissue foundon biopsies from melanoma (n = 2) and ovarian cancer (n = 1) metastases. Mean patient age was 66.2 years. Male = 5, Female = 6. CRC = colorectal cancer, HCC = hepatocellularcarcinoma, EC = Endometrial cancer. Vascular network metrics are: mean and standard deviation of blood velocity, 𝑣𝑚 and 𝑣𝑠 ; mean and standard deviation of the VFR, 𝑞𝑚 and𝑞𝑠* ; apparent network branching 𝐴𝑁𝐵; mean radius 𝑟𝑚 ; mean segment length 𝑆𝐿**𝑚 ; mean path length 𝑃 𝐿𝑚 ; the number of input/output (I/O) paths and the network dimensions.The dimensions have been indicated by two metrics, namely the actual Network Size (maximum euclidean distance between any pair of nodes), and the total number of segments.For ech metric (beyond those describing the network dimensions), the mean and the standard deviation (in bracket) over the 100 realisations of each network (10 input/outputnode combinations × 10 input VFRs) are reported.
表1 本研究生成的血管網絡及其相應微血管特性匯總 ? 非癌性網絡取自黑色素瘤(n=2)和卵巢癌(n=1)轉移灶活檢樣本中的非癌性肝組織。患者平均年齡66.2歲,男性5例,女性6例。CRC=結直腸癌,HCC=肝細胞癌,EC=子宮內膜癌。血管網絡指標包括:血流速度均值及標準差(𝑣𝑚、𝑣𝑠);體積流量率均值及標準差(𝑞𝑚、𝑞𝑠);表觀網絡分支指數(𝐴𝑁𝐵);平均半徑(𝑟𝑚);平均節段長度(𝑆𝐿𝑚);平均路徑長度(𝑃𝐿𝑚);輸入/輸出(I/O)路徑數量及網絡維度。網絡維度通過兩項指標表示:實際網絡尺寸(任意節點對之間的最大歐氏距離)和總節段數。對于每個指標(除描述網絡維度的指標外),報告每個網絡100次實現(10個輸入/輸出節點組合×10個輸入VFR)的均值和標準差(括號內)。

Table 2Summary of healthy volunteers’ demographics (age in years, sex) and trends of microvascular metrics 𝑓𝑉 , 𝐷? , 𝑣𝑚 , 𝑣𝑠 and 𝐴𝑁𝐵 within the manually-segmented ROIs (mean andstandard deviation). For sex, F indicated female, while M male. For the acquisition on the 1.5T system, routine IVIM metrics 𝑓𝑉 and 𝐷? were obtained at fixed diffusion time, onthe dMRI scan with the shortest TE
表2 健康志愿者人口統計學特征(年齡、性別)及手動分割感興趣區(ROI)內微血管指標 𝑓𝑉、𝐷?、𝑣𝑚、𝑣𝑠 和 𝐴𝑁𝐵 的趨勢總結(均值和標準差)。性別中,F 表示女性,M 表示男性。對于1.5T系統采集的數據,常規IVIM指標 𝑓𝑉 和 𝐷? 是在固定擴散時間下,從最短TE的dMRI掃描中獲取的。

Table 3Summary of patients’ demographics and key clinical data (primary cancer type, location of the imaged tumours, patients’ sex and age, in years) and trends of microvascular metrics𝑓𝑉* , 𝐷? , *𝑣𝑚* , 𝑣**𝑠 and 𝐴𝑁𝐵 within the manually-segmented tumours (mean and standard deviation). For sex, F indicated female, while M male. Routine IVIM metrics 𝑓𝑉 and 𝐷?were obtained at fixed diffusion time, on the dMRI scan with the shortest TE
表3 患者人口統計學及關鍵臨床數據(原發癌類型、成像腫瘤位置、患者性別和年齡)匯總,以及手動分割腫瘤內微血管指標𝑓𝑉、𝐷?、𝑣𝑚、𝑣𝑠和𝐴𝑁𝐵的趨勢(均值和標準差)。性別中F代表女性,M代表男性。常規IVIM指標𝑓𝑉和𝐷?是在固定擴散時間、最短TE的dMRI掃描中獲得的。




)







-IDEA集成調試配置)



)


JDK JVM)